Digital Obesity Care Reaches Socioeconomically Diverse Patients
In a real-world cohort of over 40,000 people living with obesity, digital care engaged patients across all socioeconomic groups, including low- and middle-income populations. However, affordability emerged as the primary driver of treatment discontinuation, with economic barriers disproportionately limiting long-term access and continuity of care.

.webp)

.svg)
Occupational Distribution in a Real-World Digital Care Population (PO4.209)
Anna Sommerfeld1, Kristofer Ringner1, Elin Skoglund1, Oliver Willacy1, Felix Wittström1, David Buchebner1, Martin Carlsson1,2
1. Yazen Health AB, Malmö, Sweden
2. Department of Medicine and Optometry, eHealth Institute, Linnaeus University, Kalmar, Sweden
INTRODUCTION
Obesity disproportionately affects individuals from lower socioeconomic backgrounds, with obesity prevalence estimated to be 70–80% higher in low- compared with high-income adults in Sweden. Access to effective obesity treatment remains uneven across socioeconomic groups, and novel pharmacological therapies are costly and not reimbursed, requiring patients to bear the full cost themselves, which may further widen existing health inequalities in long-term treatment outcomes. While digital care models may improve access and continuity of care, the socioeconomic and occupational profiles of patients treated within digital obesity care remain insufficiently explored.
METHODS
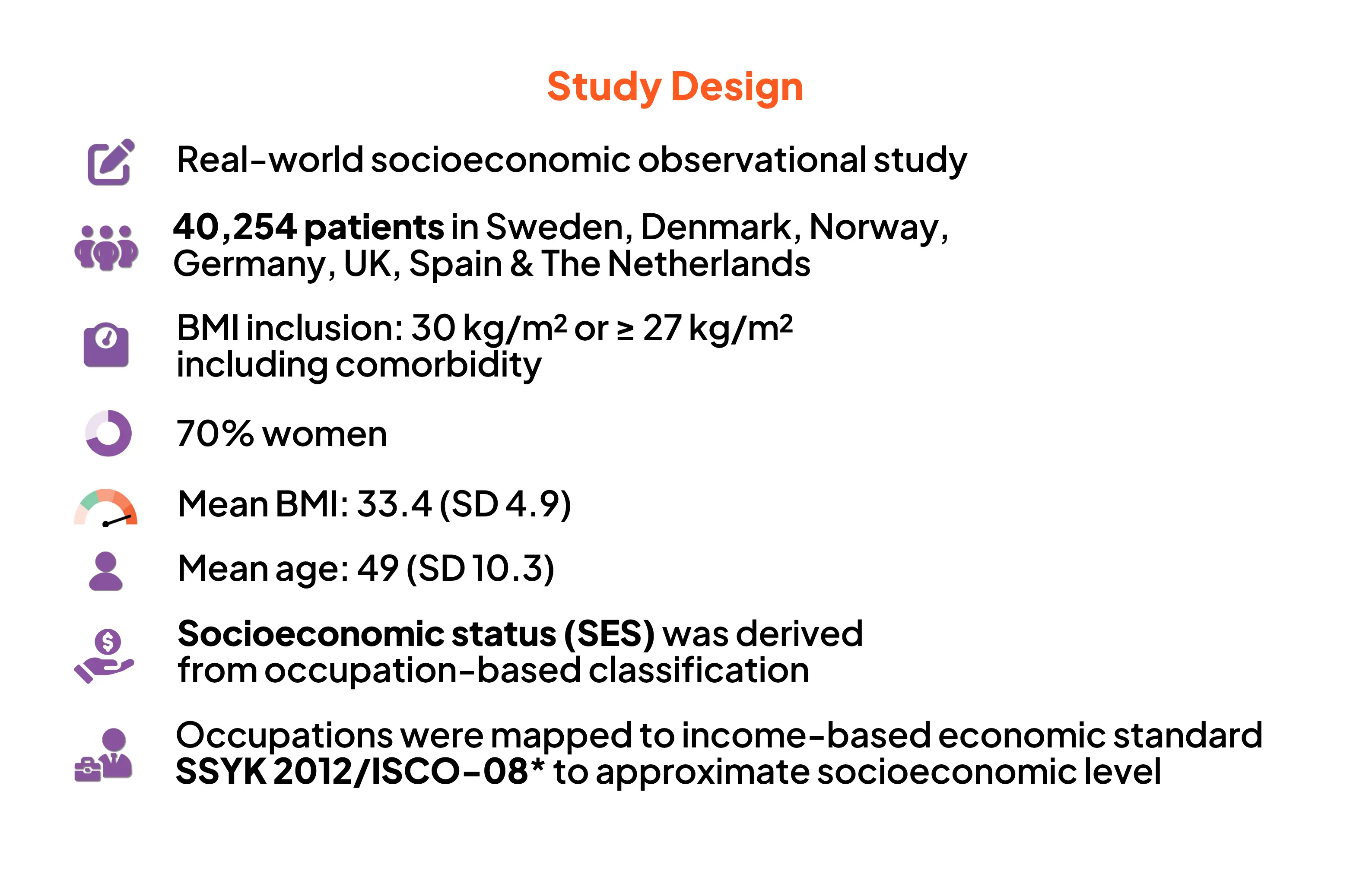
The study population comprised 40,254 Swedish adults living with obesity (mean initial BMI 33.4 kg/m²; mean age 49 years; 70% women) receiving care at Yazen Health, a licensed private Swedish healthcare provider offering a multidisciplinary digital obesity care model for people with obesity.
Occupational data were used as a proxy for socioeconomic status and classified according to the Swedish Standard Classification of Occupations (SSYK 2012) and ISCO-08 major groups. Patients were categorised into low-, middle-, or high-income groups; individual income data were not available. Formal SSYK-based classifications were retained for income grouping and health economic analyses. Self-reported reasons for treatment discontinuation were analysed descriptively. Managers within healthcare were classified as healthcare professionals to reflect healthcare training and domain expertise, while managers in other occupational groups were classified by managerial function.
RESULTS
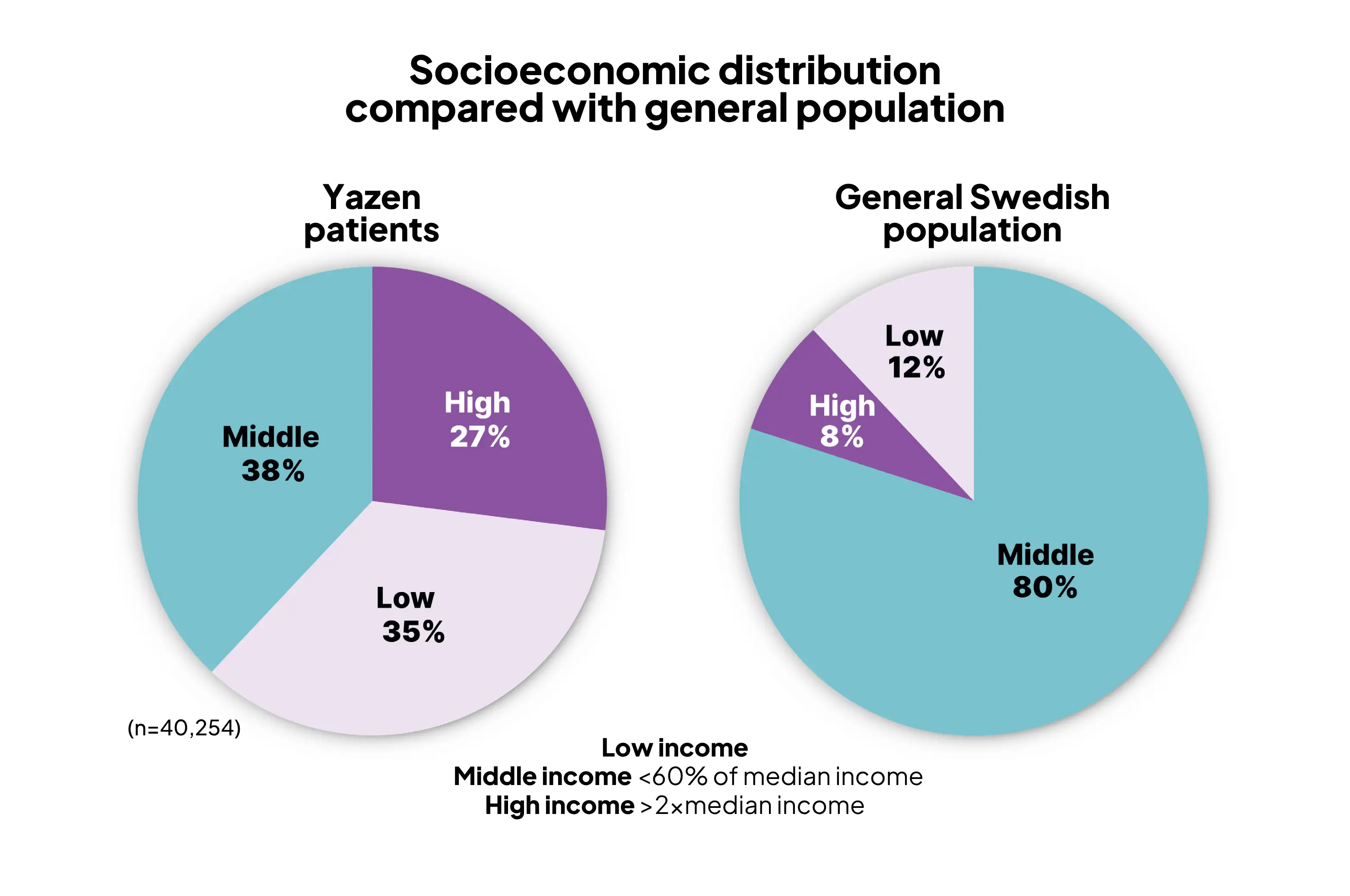
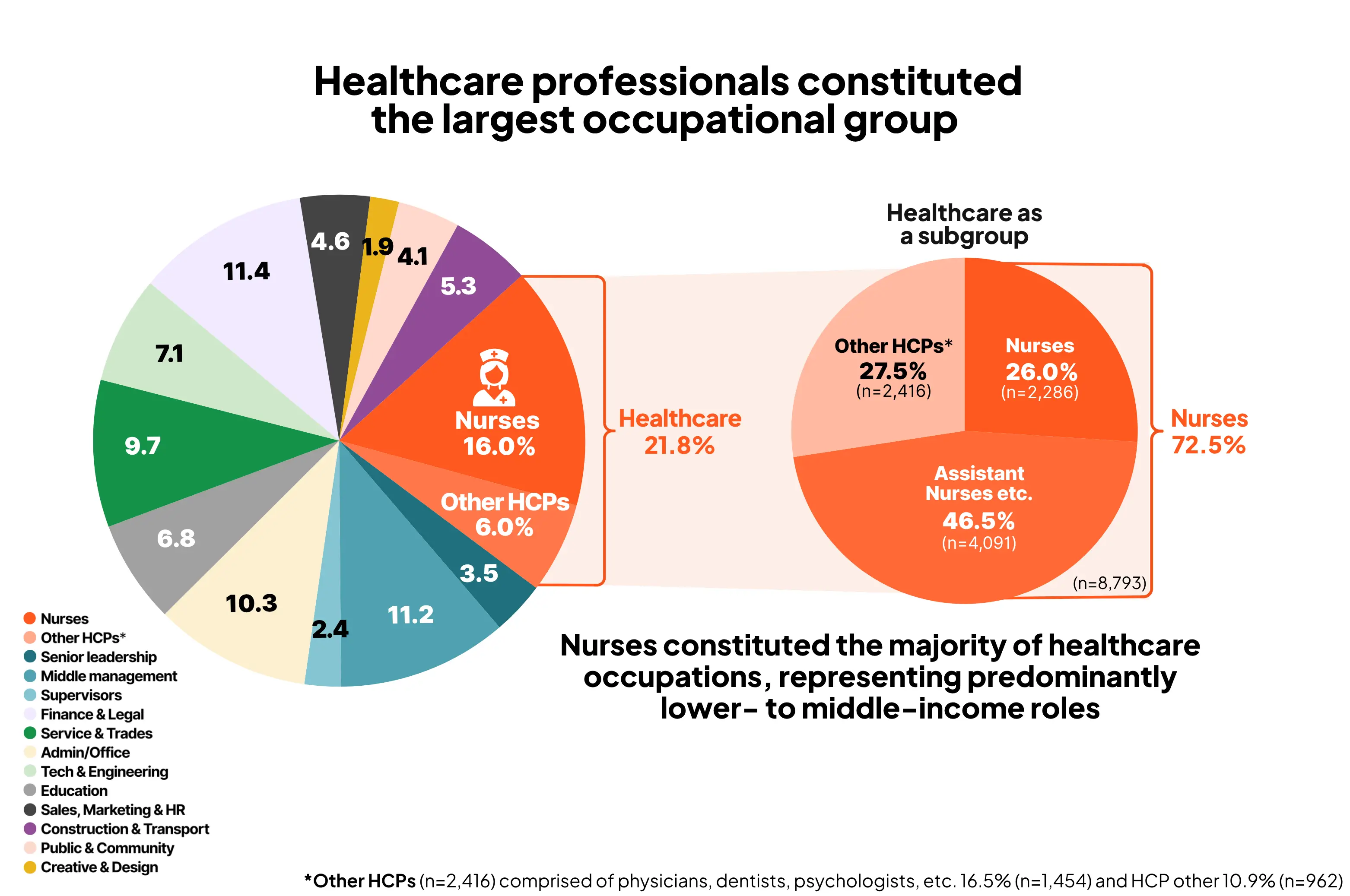
Based on occupation-derived socioeconomic grouping, 35% of patients were classified as low-income, 38% as middle-income, and 27% as high-income, compared with approximately 12%, 80%, and 8% in the general Swedish population, respectively, according to income-based economic standard (Statistics Sweden, SCB). Healthcare professionals constituted the largest occupational group (21.8%), with nurses and nurse assistants accounting for 72.5% of this group (15.9% of the total population), representing predominantly lower- to middle-income occupations. Approximately 25% of patients discontinued treatment, and 12.4% subsequently re-entered care. Economic reasons were the most frequently reported cause of discontinuation (40.9%). Return to treatment was most common among high-income individuals (61.6%), whereas discontinuation was more often permanent among low- and middle-income patients, with only 8.2% and 30.7% returning, respectively.
CONCLUSION
Digital obesity care models can engage socioeconomically diverse and traditionally underserved populations, even within entirely self-funded care settings. However, affordability emerges as a key determinant of sustained access to obesity care, with economic barriers disproportionately limiting long-term treatment continuity among lower-income patients.
Digital care can reach socioeconomically diverse populations.
Affordability is a key determinant of long-term access.
Findings support the need for:
- Reimbursement
- Targeted financial support
- Equity-Focused Obesity Policies
References:


May 11, 2026
June 19, 2026
Start din vekttapsreise med Yazen i dag
Alt du trenger å gjøre er å opprette en konto og svare på noen spørsmål om helsen din
.svg)
.svg)
Flere artikler
.webp)

Yazen-modellen – Moderne fedmebehandling levert via en digital omsorgsmodell. En beskrivende analyse
Yazen-modellen går utover tradisjonelle metoder og gir pasientene verktøyene de trenger for å håndtere sykdommen, ved å adressere medisinske og atferdsmessige aspekter, utdanning og sosial støtte via en digital plattform som tilbyr tilgjengelig, kontinuerlig og effektiv vektreduksjon og vekthåndtering.
.webp)
Høy etterlevelse av GLP-1-reseptoragonister: 18-månedersresultater fra Yazen-modellen
Høy etterlevelse av GLP-1-reseptoragonister innenfor et strukturert, digitalt basert vekthåndteringsprogram kan bidra til bedre langtids etterlevelse av legemiddelbehandling.
Sammendrag
Denne virkelighetsnære analysen fra Yazens første storskala operasjonelle kvalitetsoppfølging viser nesten 70 % etterlevelse av GLP-1-legemidler etter 12 måneder, noe som overgår tidligere studier som har vist 20–50 %¹–⁴.
Resultater med tirzepatid og semaglutid i klinisk praksis hos over 40 000 pasienter
Varig vektnedgang i den virkelige verden hos mer enn 40 000 pasienter
Betydelig vektnedgang ble oppnådd med GLP-1-basert behandling som en del av en omfattende, digital behandlingsmodell for fedme. Resultatene ble opprettholdt i opptil 24 måneder, med 57 % av pasientene fortsatt i behandling, noe som demonstrerer sterk langsiktig effektivitet i klinisk praksis.