Digital Obesity Care Reaches Socioeconomically Diverse Patients
In a real-world cohort of over 40,000 people living with obesity, digital care engaged patients across all socioeconomic groups, including low- and middle-income populations. However, affordability emerged as the primary driver of treatment discontinuation, with economic barriers disproportionately limiting long-term access and continuity of care.

.webp)

.svg)
Occupational Distribution in a Real-World Digital Care Population (PO4.209)
Anna Sommerfeld1, Kristofer Ringner1, Elin Skoglund1, Oliver Willacy1, Felix Wittström1, David Buchebner1, Martin Carlsson1,2
1. Yazen Health AB, Malmö, Sweden
2. Department of Medicine and Optometry, eHealth Institute, Linnaeus University, Kalmar, Sweden
INTRODUCTION
Obesity disproportionately affects individuals from lower socioeconomic backgrounds, with obesity prevalence estimated to be 70–80% higher in low- compared with high-income adults in Sweden. Access to effective obesity treatment remains uneven across socioeconomic groups, and novel pharmacological therapies are costly and not reimbursed, requiring patients to bear the full cost themselves, which may further widen existing health inequalities in long-term treatment outcomes. While digital care models may improve access and continuity of care, the socioeconomic and occupational profiles of patients treated within digital obesity care remain insufficiently explored.
METHODS
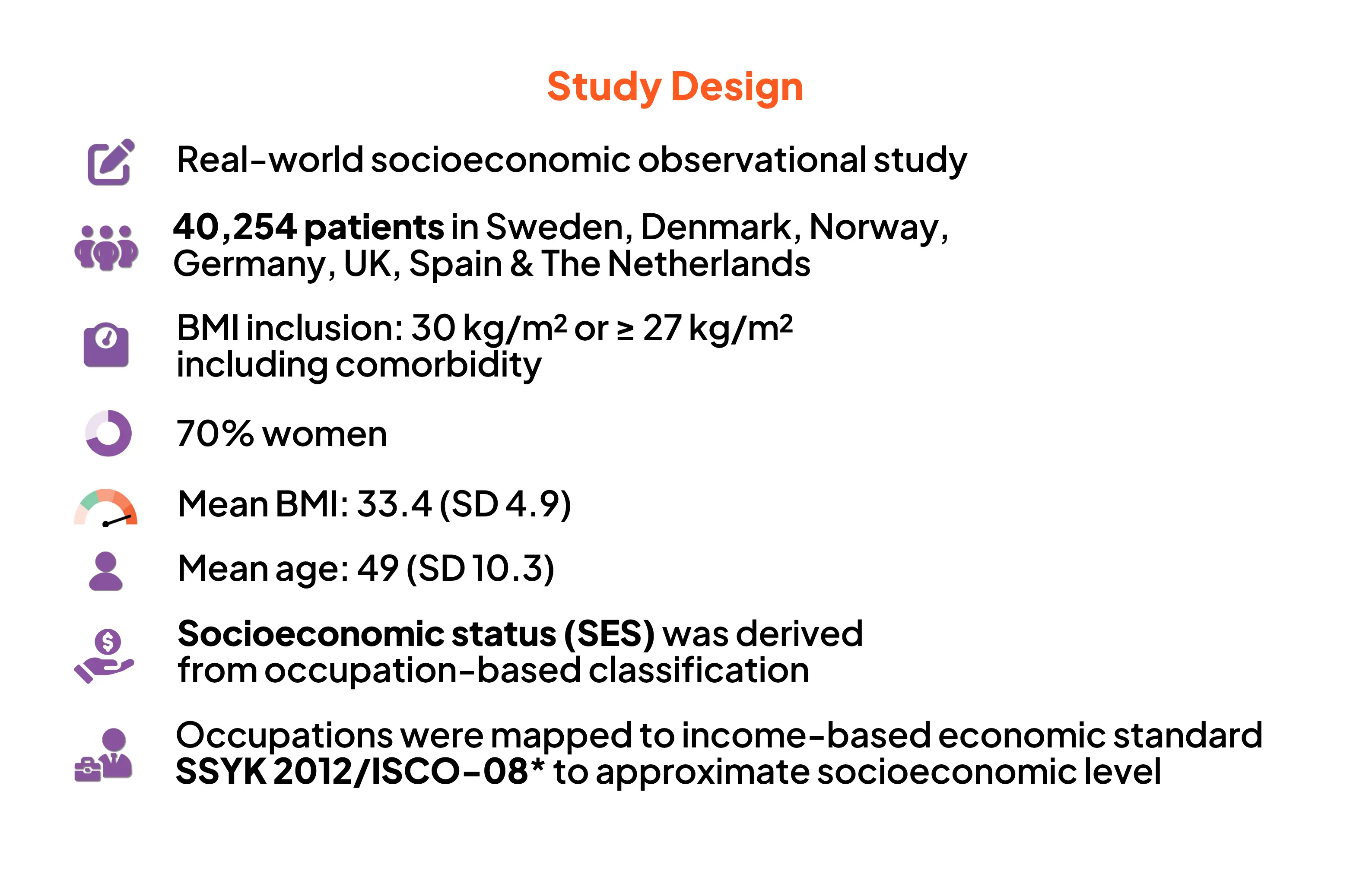
The study population comprised 40,254 Swedish adults living with obesity (mean initial BMI 33.4 kg/m²; mean age 49 years; 70% women) receiving care at Yazen Health, a licensed private Swedish healthcare provider offering a multidisciplinary digital obesity care model for people with obesity.
Occupational data were used as a proxy for socioeconomic status and classified according to the Swedish Standard Classification of Occupations (SSYK 2012) and ISCO-08 major groups. Patients were categorised into low-, middle-, or high-income groups; individual income data were not available. Formal SSYK-based classifications were retained for income grouping and health economic analyses. Self-reported reasons for treatment discontinuation were analysed descriptively. Managers within healthcare were classified as healthcare professionals to reflect healthcare training and domain expertise, while managers in other occupational groups were classified by managerial function.
RESULTS
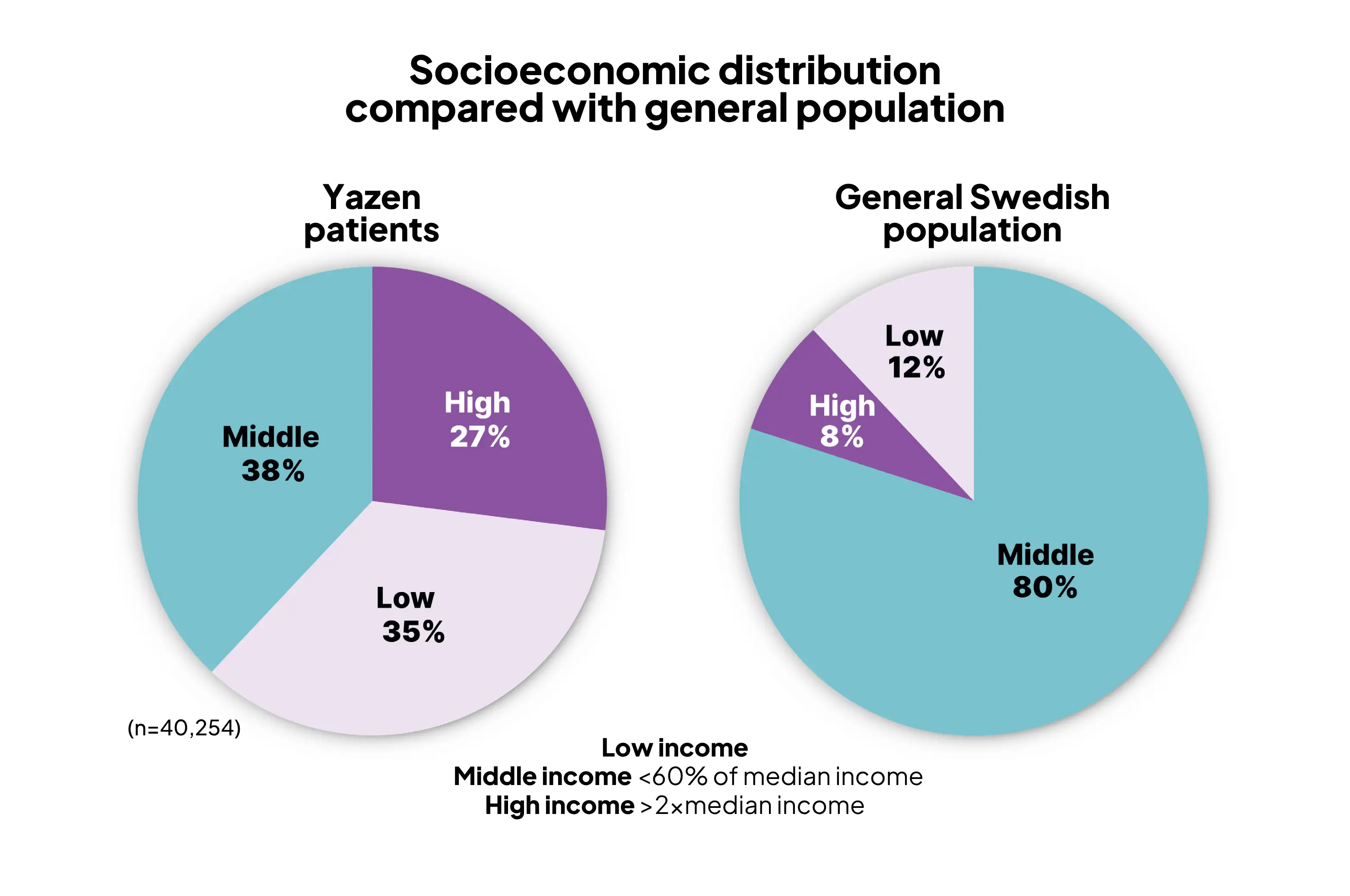
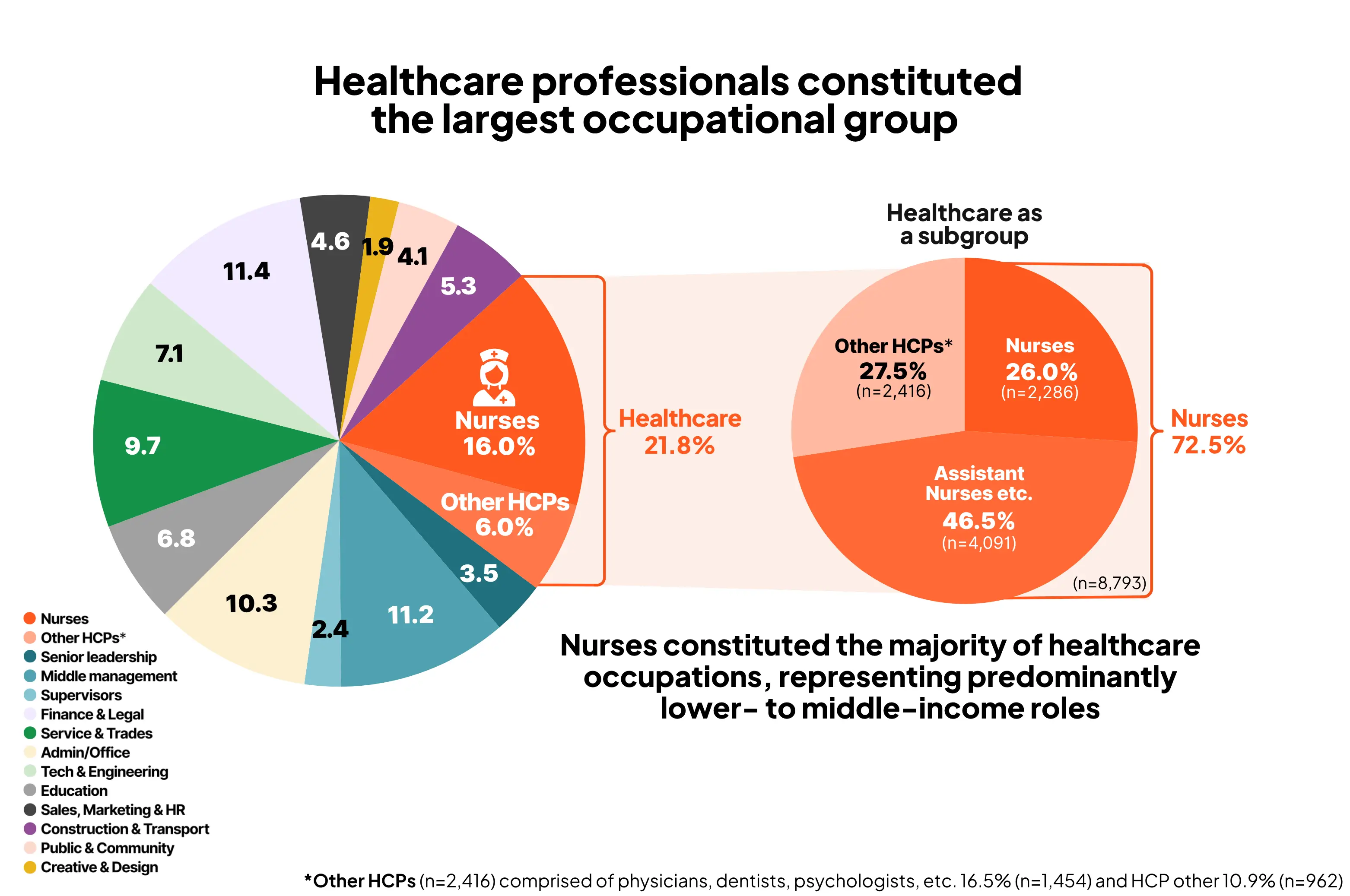
Based on occupation-derived socioeconomic grouping, 35% of patients were classified as low-income, 38% as middle-income, and 27% as high-income, compared with approximately 12%, 80%, and 8% in the general Swedish population, respectively, according to income-based economic standard (Statistics Sweden, SCB). Healthcare professionals constituted the largest occupational group (21.8%), with nurses and nurse assistants accounting for 72.5% of this group (15.9% of the total population), representing predominantly lower- to middle-income occupations. Approximately 25% of patients discontinued treatment, and 12.4% subsequently re-entered care. Economic reasons were the most frequently reported cause of discontinuation (40.9%). Return to treatment was most common among high-income individuals (61.6%), whereas discontinuation was more often permanent among low- and middle-income patients, with only 8.2% and 30.7% returning, respectively.
CONCLUSION
Digital obesity care models can engage socioeconomically diverse and traditionally underserved populations, even within entirely self-funded care settings. However, affordability emerges as a key determinant of sustained access to obesity care, with economic barriers disproportionately limiting long-term treatment continuity among lower-income patients.
Digital care can reach socioeconomically diverse populations.
Affordability is a key determinant of long-term access.
Findings support the need for:
- Reimbursement
- Targeted financial support
- Equity-Focused Obesity Policies
References:


May 11, 2026
June 19, 2026
Comience su viaje de pérdida de peso con Yazen hoy
Todo lo que necesita hacer es crear una cuenta y responder algunas preguntas sobre su salud
.svg)
.svg)
Más artículos


Pérdida de peso sostenible y beneficios para la salud en el cuidado de la obesidad: Resultados de la evaluación en el mundo real de 18 meses en un entorno de atención virtual del primer seguimiento de calidad operativa de Yazens
Este análisis de datos de evaluación en situaciones reales de 18 meses demuestra que el modelo de atención totalmente digital de Yazen Health, que integra tratamiento farmacológico e intervención en el estilo de vida, puede ofrecer resultados efectivos y sostenibles en un entorno real.
Resumen
Los pacientes lograron una reducción de peso del 16,6 %, acompañada de mejoras en los marcadores de salud metabólica, incluyendo los valores de laboratorio, a pesar de las limitaciones en el suministro de medicamentos y sin usar la dosis máxima recomendada de semaglutida. El 70 % permaneció en el programa después de 12 meses. Los resultados de pérdida de peso fueron comparables a los observados en ECA como los ensayos STEP1-2.
.webp)
El Modelo Yazen – Tratamiento moderno de la obesidad proporcionado mediante un modelo de atención digital. Un análisis descriptivo
El Modelo Yazen permite un tratamiento moderno de la obesidad integrando tratamiento médico, intervención en el estilo de vida y apoyo social. Hasta ahora*, más de 30 000 pacientes han recibido tratamiento mediante este modelo.
Resumen
El Modelo Yazen va más allá de los métodos tradicionales y proporciona a los pacientes las herramientas necesarias para gestionar su enfermedad abordando los aspectos médicos y conductuales, la educación y el apoyo social mediante una plataforma digital que permite una pérdida de peso accesible, continua y eficaz.
.webp)
Yazen en el Congreso Europeo de Obesidad (ECO) 2025: Liderando el tratamiento moderno de la obesidad a través de la innovación digital
En ECO 2025 en Málaga, Yazen presentó soluciones digitales y estrategias personalizadas que están revolucionando el manejo de la obesidad y mejorando los resultados clínicos.