Digital Obesity Care Reaches Socioeconomically Diverse Patients
In a real-world cohort of over 40,000 people living with obesity, digital care engaged patients across all socioeconomic groups, including low- and middle-income populations. However, affordability emerged as the primary driver of treatment discontinuation, with economic barriers disproportionately limiting long-term access and continuity of care.

.webp)

.svg)
Occupational Distribution in a Real-World Digital Care Population (PO4.209)
Anna Sommerfeld1, Kristofer Ringner1, Elin Skoglund1, Oliver Willacy1, Felix Wittström1, David Buchebner1, Martin Carlsson1,2
1. Yazen Health AB, Malmö, Sweden
2. Department of Medicine and Optometry, eHealth Institute, Linnaeus University, Kalmar, Sweden
INTRODUCTION
Obesity disproportionately affects individuals from lower socioeconomic backgrounds, with obesity prevalence estimated to be 70–80% higher in low- compared with high-income adults in Sweden. Access to effective obesity treatment remains uneven across socioeconomic groups, and novel pharmacological therapies are costly and not reimbursed, requiring patients to bear the full cost themselves, which may further widen existing health inequalities in long-term treatment outcomes. While digital care models may improve access and continuity of care, the socioeconomic and occupational profiles of patients treated within digital obesity care remain insufficiently explored.
METHODS
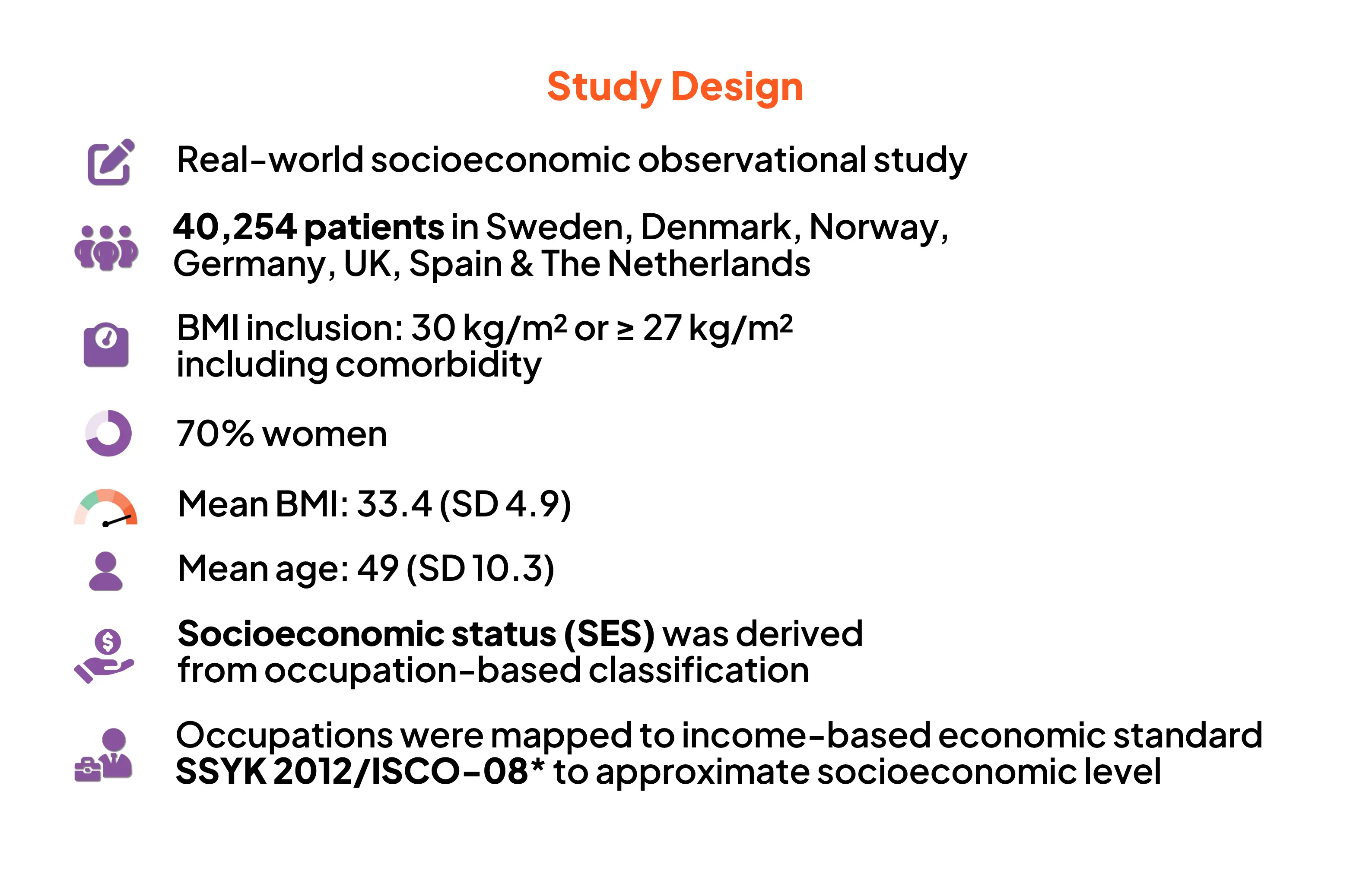
The study population comprised 40,254 Swedish adults living with obesity (mean initial BMI 33.4 kg/m²; mean age 49 years; 70% women) receiving care at Yazen Health, a licensed private Swedish healthcare provider offering a multidisciplinary digital obesity care model for people with obesity.
Occupational data were used as a proxy for socioeconomic status and classified according to the Swedish Standard Classification of Occupations (SSYK 2012) and ISCO-08 major groups. Patients were categorised into low-, middle-, or high-income groups; individual income data were not available. Formal SSYK-based classifications were retained for income grouping and health economic analyses. Self-reported reasons for treatment discontinuation were analysed descriptively. Managers within healthcare were classified as healthcare professionals to reflect healthcare training and domain expertise, while managers in other occupational groups were classified by managerial function.
RESULTS
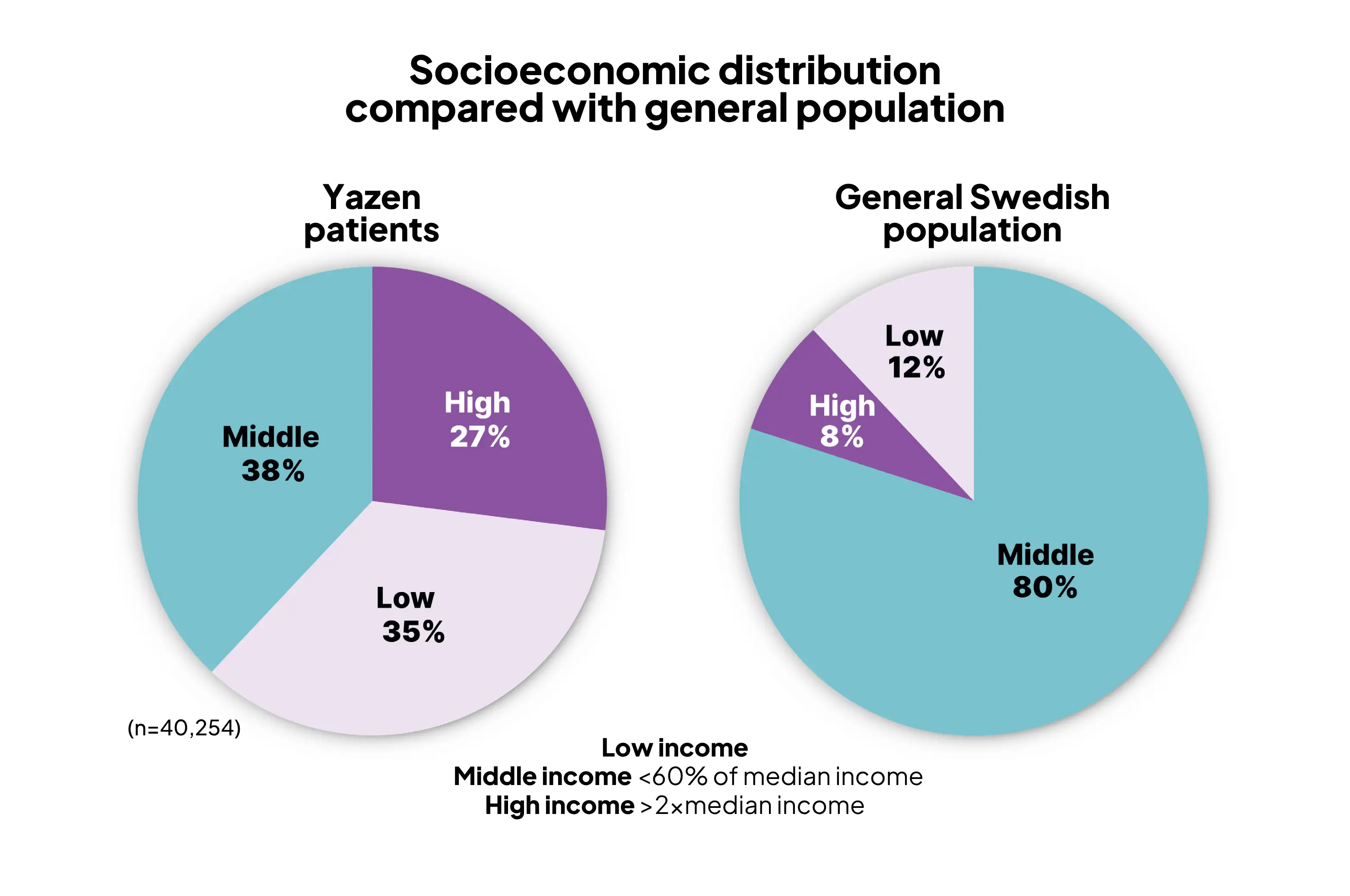
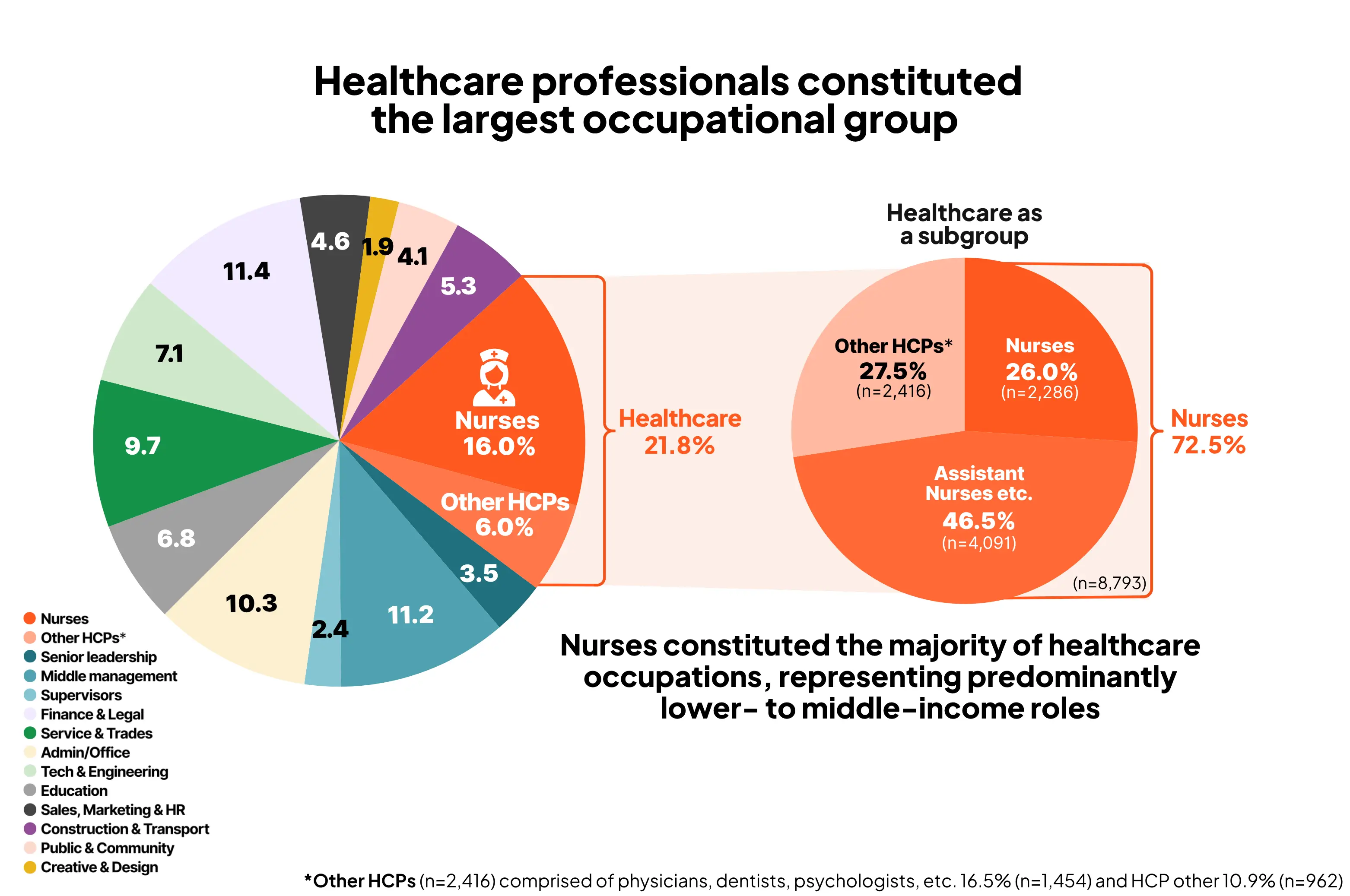
Based on occupation-derived socioeconomic grouping, 35% of patients were classified as low-income, 38% as middle-income, and 27% as high-income, compared with approximately 12%, 80%, and 8% in the general Swedish population, respectively, according to income-based economic standard (Statistics Sweden, SCB). Healthcare professionals constituted the largest occupational group (21.8%), with nurses and nurse assistants accounting for 72.5% of this group (15.9% of the total population), representing predominantly lower- to middle-income occupations. Approximately 25% of patients discontinued treatment, and 12.4% subsequently re-entered care. Economic reasons were the most frequently reported cause of discontinuation (40.9%). Return to treatment was most common among high-income individuals (61.6%), whereas discontinuation was more often permanent among low- and middle-income patients, with only 8.2% and 30.7% returning, respectively.
CONCLUSION
Digital obesity care models can engage socioeconomically diverse and traditionally underserved populations, even within entirely self-funded care settings. However, affordability emerges as a key determinant of sustained access to obesity care, with economic barriers disproportionately limiting long-term treatment continuity among lower-income patients.
Digital care can reach socioeconomically diverse populations.
Affordability is a key determinant of long-term access.
Findings support the need for:
- Reimbursement
- Targeted financial support
- Equity-Focused Obesity Policies
References:


May 11, 2026
June 19, 2026
Begin vandaag nog met afvallen met Yazen
Het enige wat je hoeft te doen is een account aanmaken en enkele vragen over je gezondheid beantwoorden.
.svg)
.svg)
Meer artikelen


Duurzaam gewichtsverlies en gezondheidsvoordelen in obesitaszorg: 18 maanden real-world evaluatieresultaten binnen een digitale zorgomgeving
Deze 18-maanden real-world analyse toont aan dat het volledig digitale zorgmodel van Yazen Health, waarin farmacologische behandeling wordt gecombineerd met leefstijlinterventies, effectieve en duurzame resultaten kan leveren in een dagelijkse zorgsetting.
Samenvatting
Patiënten realiseerden een gemiddeld gewichtsverlies van 16,6%, met gelijktijdige verbeteringen in metabole gezondheidsmarkers, waaronder laboratoriumwaarden. Dit werd bereikt ondanks beperkingen in medicijnbeschikbaarheid en zonder gebruik van de maximale aanbevolen dosis semaglutide. 70% van de patiënten bleef na 12 maanden in het programma. De resultaten zijn vergelijkbaar met uitkomsten uit RCT’s zoals de STEP-trials¹-².
.webp)
Hoge therapietrouw bij GLP-1-receptoragonisten: 18-maanden uitkomsten van het Yazen-model
Hoge therapietrouw aan GLP-1-receptoragonisten binnen een gestructureerd, digitaal ondersteund behandelprogramma kan bijdragen aan betere medicatietrouw op de lange termijn.
Samenvatting
Deze real-world analyse uit Yazens eerste grootschalige operationele kwaliteitsopvolging toont aan dat bijna 70% van de patiënten na 12 maanden nog steeds hun GLP-1-medicatie gebruikte, aanzienlijk hoger dan eerdere studies, die therapietrouwpercentages van 20–50% rapporteerden¹–⁴. Na 2 jaar* was 60% van de patiënten nog steeds in behandeling.
.webp)
Het Yazen-model – Moderne obesitasbehandeling via een digitaal zorgmodel: een descriptieve analyse
Het Yazen-model maakt moderne obesitaszorg mogelijk door medische behandeling, leefstijlinterventie en sociale ondersteuning te integreren. Inmiddels* hebben meer dan 30.000 patiënten een behandeling gevolgd via dit model.
Samenvatting
Het Yazen-model gaat verder dan traditionele behandelmethoden. Het biedt patiënten de benodigde tools om hun aandoening te beheersen door zowel medische als gedragsmatige aspecten aan te pakken, aangevuld met educatie en sociale steun. Dit alles wordt aangeboden via één digitaal platform, waardoor de behandeling toegankelijk, continu en effectief is voor duurzaam gewichtsverlies en -behoud.